The information presented here outlines general characteristics of each
disorder. Presentation of signs and symptoms may vary from patient to patient.
Cutaneous Mastocytosis
Cutaneous mastocytosis (CM) is a form of mastocytosis that affects the skin, with no
evidence of systemic mast cell involvement, in primarily pediatric patients.1-3
Please note: Most patients diagnosed with CM are children, whereas SM is usually diagnosed in
adults.2-4 Adults with skin lesions
may receive a provisional
diagnosis of mastocytosis in the skin prior to undergoing complete staging, including bone marrow
analysis, to confirm/exclude CM or SM.4,5
Common Signs and Symptoms
| ISM |
CM |
| DERMATOLOGIC |

Darier sign: Elicited upon stroking of lesioned
skin1,2
Darier sign: Elicited upon stroking of lesioned
skin1,2
|

Monomorphic maculopapular lesions, round, brown or red in color arise
predominantly on the thigh and trunk. Lesions may spread or spontaneously disappear, which
may or may not
indicate disease progression1,2,7
Symptoms such as flushing, pruritus, and positive Darier sign may be
observed1,7,8
|
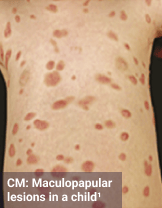
Maculopapular CM, previously known as urticaria pigmentosa, is typically
characterized by round brown or red skin lesions1,2
Polymorphic, larger lesions, may present
initially with nodules or plaques, and
typically arise on the trunk, head, and extremities; presents in
children1,2
Monomorphic, small round lesions may be
present in a small subset of patients,
including
children1,2,9
|
|
|

Diffuse CM (DCM), characterized by
generalized erythema with a brown or yellow
tint and thickened
skin. Pronounced dermographism and blisters can be
associated
with DCM as well1,2
|
|
|

Mastocytoma, typically presents as 1-3
brown
or red nodular lesions and may
initially be associated with
blisters1,2
These lesions or blisters can be isolated or multilocalized9
|
| GASTROINTESTINAL |
GI involvement is commonly reported in patients with ISM7,10,11
Symptoms may include diarrhea, abdominal cramping, bloating,
nausea, and vomiting7,11,12
|
|
| SYSTEMIC |
Systemic symptoms include fatigue, anaphylaxis, and weight loss7,11-13
Anaphylaxis may occur; patients typically present with hypotensive
syncope and without flushing, urticaria, pruritus, and
angioedema7,9,14
Episodes of anaphylaxis appear more likely to develop in patients with mastocytosis
compared to the general population; Hymenoptera
stings are a
common trigger7,15,16
|
Anaphylaxis is uncommon but may be possible1,2,17
|
| OTHER |
Additional symptoms such as cognitive impairment, dizziness,
headache, osteoporosis, musculoskeletal pain, breathing difficulties,
anxiety, or depression may occur7,12,13,18
Please note that this list is not inclusive of all symptoms patients with
ISM may experience
|
Involvement is most commonly seen in the skin1,2
|
Additional Considerations
This section provides some information that may be helpful in further
identifying patients with ISM vs CM and is not inclusive of all distinguishing features. Please refer to
the formal guidelines for each disorder, if available, for a more comprehensive list.

In pediatric patients, the typical course of CM is usually temporary and often resolves spontaneously
around puberty, whereas
ISM in adults is usually chronic.1,2
The information presented here outlines general characteristics of each
disorder. Presentation of signs and symptoms may vary from patient to patient.
Chronic Spontaneous Urticaria
Chronic spontaneous urticaria (CSU) is a spontaneous appearance of urticaria, defined
as wheals (hives), angioedema, or both for >6 weeks
due to known or unknown
causes.1,2
Common Signs and Symptoms
| ISM |
CSU |
| DERMATOLOGIC |

Monomorphic maculopapular lesions, round, brown or red in color arise
predominantly on the thigh and trunk.
Lesions may spread or
spontaneously disappear, which may or may not indicate disease progression4-6
Symptoms such as flushing, pruritus, and positive Darier sign may be
observed4,6,7
The Darier sign is an important clinical feature of mastocytosis skin
lesions. It is defined by the development of a
wheal-and-flare reaction upon
mechanical irritation of the
lesion4-6
|

Wheals are defined by swelling and
erythema
of varying size and shape,
presenting with itching or burning.
Wheals
are transient and may resolve within 30
minutes to 24 hours1,2
Angioedema is characterized by sudden
swelling or erythema in
the deep layers of the
dermis, usually with sensation of
tingling,
burning, tightness, and pain. Resolution of
angioedema is slower than wheals and may
take up to 72 hours1,8
|
| GASTROINTESTINAL |
GI involvement is commonly reported in patients with ISM6,9,10
Symptoms may include diarrhea, abdominal cramping, bloating,
nausea, and vomiting6,10,11
|
Some patients can have GI symptoms such as nausea, vomiting,
and epigastric abdominal pain12
|
| SYSTEMIC |
Systemic symptoms include fatigue, anaphylaxis, and weight loss6,10,11,13
Anaphylaxis may occur; patients typically present with hypotensive syncope and without
flushing, urticaria, pruritus, and angioedema6,14,15
Episodes of anaphylaxis appear more likely to develop in patients with mastocytosis
compared to the general population; Hymenoptera stings are a common
trigger6,16,17
|
|
| OTHER |
Additional symptoms such as cognitive impairment, dizziness,
headache, osteoporosis, musculoskeletal pain, breathing difficulties, anxiety, or depression
may occur6,11,13,18
Please note that this list is not inclusive of all symptoms patients with
ISM may experience
|
Some additional manifestations such as Kounis syndrome, hypertension, striatum dysfunction,
respiratory symptoms, arthritis, arthralgia, or osteoporosis may occur12
|
Additional Considerations
This section provides some information that may be helpful in further
identifying patients with ISM vs CSU and is not inclusive of all distinguishing features. Please refer
to the formal guidelines for each disorder, if available, for a more comprehensive list.
CSU may occur with daily/almost daily signs and symptoms or as an intermittent/recurrent course. CSU
may also recur after
months or years of full remission. ISM is usually
chronic.1,19
The information presented here outlines general characteristics of each
disorder. Presentation of signs and symptoms may vary from patient to patient.
Mast Cell Activation Syndrome
Mast cell activation syndromes (MCAS) are a clustering of disorders characterized by
the accumulation of MCs in tissues and organs,
and/or release of MC
mediators, with symptoms related to MC degranulation and mediator release.1 MCAS can be divided
into primary,
secondary, and idiopathic.2,3 Primary MCAS or
monoclonal MCAS (mMCAS) is characterized by lack of cutaneous findings and presence of
KIT D816V mutation or expression of CD25 in MCs.3
Common Signs and Symptoms
| ISM |
MCAS/mMCAS |
| DERMATOLOGIC |

ISM: Maculopapular lesions in an adult4
Monomorphic maculopapular lesions, round, brown or red in color arise
predominantly on the thigh and trunk. Lesions may spread or spontaneously disappear, which
may or may not indicate disease progression5-7
Symptoms such as flushing, pruritus, and positive Darier sign may be
observed5,7,8
The Darier sign is an important clinical feature of mastocytosis skin
lesions. It is defined by the development of a
wheal-and-flare reaction upon mechanical irritation of the
lesion5-7
|
Episodic symptoms such as pruritus, urticaria, and flushing
may occur2,9,10
|
| GASTROINTESTINAL |
GI involvement is commonly reported in patients with ISM7,11,12
Symptoms may include diarrhea, abdominal cramping, bloating,
nausea, and vomiting7,12,13
|
Patients may present with nausea, vomiting, cramping
abdominal pain, and diarrhea1,3
|
| SYSTEMIC |
Systemic symptoms include fatigue, anaphylaxis, and weight loss7,12-14
Anaphylaxis may occur; patients typically present with hypotensive syncope and without
flushing, urticaria, pruritus, and angioedema7,15,16
Episodes of anaphylaxis appear more likely to develop in patients with mastocytosis
compared to the general population; Hymenoptera stings are a common
trigger7,17,18
|
During episodes of anaphylaxis, cardiovascular, respiratory,
dermatologic, and GI organ systems are often affected. Symptoms
include urticaria, flushing, pruritus, abdominal cramping,
nausea,
diarrhea, wheezing, shortness of breath, syncope,
and hypotension1,10
|
| OTHER |
Additional symptoms such as cognitive impairment, dizziness,
headache, osteoporosis, musculoskeletal pain, breathing difficulties, anxiety, or depression
may occur7,13,14,19
Please note that this list is not inclusive of all symptoms patients
with ISM may experience
|
Chronic urticaria and angioedema can be a feature of secondary and idiopathic
MCAS3
Additional symptoms such as headache, tachycardia, and fatigue
may occur1,9,10
|
Additional Considerations
This section provides some information that may be helpful in further
identifying patients with ISM vs MCAS and is not inclusive of all distinguishing features. Please refer
to the formal guidelines for each disorder, if available, for a more comprehensive list.

Basal serum tryptase levels in patients with MCAS/mMCAS are usually normal or mildly increased. If
patients with suspected MC disorders
have elevated tryptase levels,
evaluation of systemic mastocytosis or hereditary alpha tryptasemia may be warranted.2,10,20
The information presented here outlines general characteristics of each
disorder. Presentation of signs and symptoms may vary from patient to patient.
Hereditary Alpha Tryptasemia
Hereditary alpha tryptasemia (HαT) is a disorder characterized by an autosomal-dominant
genetic trait with extra copies of the
TPSAB1 gene, which encodes
α-tryptase.1-3 HαT is associated with elevated baseline serum tryptase levels (>8
ng/mL).1-3
Common Signs and Symptoms
| ISM |
HαT |
| DERMATOLOGIC |

ISM: Maculopapular lesions in an adult4
Monomorphic maculopapular lesions, round, brown or red in color arise
predominantly on the thigh and trunk. Lesions may spread or spontaneously disappear, which
may or may not indicate disease progression5-7
Symptoms such as flushing, pruritus, and positive Darier sign may be
observed5,7,8
The Darier sign is an important clinical feature of mastocytosis skin
lesions. It is defined by the development of a
wheal-and-flare reaction upon
mechanical irritation of the
lesion5-7
|
Typically characterized by recurrent cutaneous symptoms,
including flushing and pruritus1,3
Angioedema and urticaria are commonly reported9,10
|
| GASTROINTESTINAL |
GI involvement is commonly reported in patients with ISM7,11,12
Symptoms may include diarrhea, abdominal cramping, bloating,
nausea, and vomiting7,12,13
|
IBS-like symptoms or symptoms of chronic gastroesophageal reflux are commonly
present1,3
|
| SYSTEMIC |
Systemic symptoms include fatigue, anaphylaxis, and weight loss7,12-14
Anaphylaxis may occur; patients typically present with hypotensive syncope and without
flushing, urticaria, pruritus, and angioedema7,15,16
Episodes of anaphylaxis appear more likely to develop in patients
with mastocytosis compared to the general population;
Hymenoptera
stings are a common trigger7,17,18
|
Systemic reaction consistent with IgE-mediated hypersensitivity
reaction or systemic venom reaction to stinging insects
(Hymenoptera) can occur3,19
|
| OTHER |
Additional symptoms such as cognitive impairment, dizziness,
headache, osteoporosis, musculoskeletal pain, breathing difficulties, anxiety, or depression
may occur7,13,14,20
Please note that this list is not inclusive of all symptoms patients with
ISM may experience
|
Dysautonomia, arthralgia, primary dentition, headache, body pain,
connective tissue abnormalities, and joint hypermobility may
occur2,3
|
Additional Considerations
This section provides some information that may be helpful in further
identifying patients with ISM vs HαT and is not inclusive of all distinguishing features. Please refer
to the formal guidelines for each disorder, if available, for a more comprehensive list.

Patients with SM may simultaneously have HαT, especially among patients with ISM and BMM. In patients
with mastocytosis, presence of
HαT can indicate increased risk and
severity for anaphylaxis.7,21-23
The information presented here outlines general characteristics of each
disorder. Presentation of signs and symptoms may vary from patient to patient.
Hypereosinophilic Syndrome
Hypereosinophilic syndrome (HES) is a heterogeneous group of rare disorders
characterized by persistently elevated eosinophil count
and
eosinophil-mediated organ damage.1,2
Common Signs and Symptoms
| ISM |
HES |
| DERMATOLOGIC |

ISM: Maculopapular lesions in an adult3
Monomorphic maculopapular lesions, round, brown or red in color arise
predominantly on the thigh and trunk. Lesions may spread or spontaneously disappear, which
may or may not indicate disease progression4-6
Symptoms such as flushing, pruritus, and positive Darier sign may be
observed4,6,7
The Darier sign is an important clinical feature of mastocytosis skin
lesions. It is defined by the development of a
wheal-and-flare reaction upon
mechanical irritation of the
lesion4-6
|
Cutaneous manifestations such as urticaria, erythema,
angioedema, ulceration, pruritus, or eczema are
common1,2
|
| GASTROINTESTINAL |
GI involvement is commonly reported in patients with ISM6,8,9
Symptoms may include diarrhea, abdominal cramping,
bloating,
nausea, and vomiting6,9,10
|
Abdominal pain, diarrhea, nausea, and vomiting1,2
Eosinophilic gastritis, enterocolitis, or colitis may be present2
|
| SYSTEMIC |
Systemic symptoms include fatigue, anaphylaxis, and weight loss6,9-11
Anaphylaxis may occur; patients typically present with hypotensive syncope and without
flushing, urticaria, pruritus, and
angioedema6,12,13
Episodes of anaphylaxis appear more likely to develop in patients with mastocytosis
compared to the general population; Hymenoptera
stings are a
common trigger6,14,15
|
Weakness, fatigue, and fever may occur1,2,16
|
| OTHER |
Additional symptoms such as cognitive impairment, dizziness,
headache, osteoporosis, musculoskeletal pain, breathing difficulties,
anxiety, or depression may occur6,10,11,17
Please note that this list is not inclusive of all symptoms patients with
ISM may experience
|
Cough, shortness of breath, myalgias, and other cardiac, neurological
and respiratory manifestations (eg, rhinitis, asthma, and
sinusitis)
may occur1,2,16
|
The information presented here outlines general characteristics of each
disorder. Presentation of signs and symptoms may vary from patient to patient.
Irritable Bowel Syndrome
Irritable bowel syndrome (IBS) is a chronic disorder of gut-brain interaction. IBS is
characterized by symptoms of recurrent abdominal pain
and disordered
defecation.1-3
Common Signs and Symptoms
| ISM |
IBS |
| DERMATOLOGIC |

ISM: Maculopapular lesions in an adult4
Monomorphic maculopapular lesions, round, brown or red in color arise
predominantly on the thigh and trunk. Lesions may spread or spontaneously disappear, which
may or may not indicate disease progression5-7
Symptoms such as flushing, pruritus, and positive Darier sign may be
observed5,7,8
The Darier sign is an important clinical feature of mastocytosis skin
lesions. It is defined by the development of a
wheal-and-flare reaction upon mechanical irritation of the lesion5-7
|
|
| GASTROINTESTINAL |
GI involvement is commonly reported in patients with ISM7,9,10
Symptoms may include diarrhea, abdominal cramping, bloating,
nausea, and vomiting7,10,11
|
Recurrent abdominal pain, change in stool frequency, diarrhea,
and/or constipation1-3
Abdominal bloating and distention are commonly reported symptoms1-3
|
| SYSTEMIC |
Systemic symptoms include fatigue, anaphylaxis, and weight loss7,10-12
Anaphylaxis may occur; patients typically present with hypotensive syncope and without
flushing, urticaria, pruritus, and angioedema7,13,14
Episodes of anaphylaxis appear more likely to develop in patients with mastocytosis
compared to the general population; Hymenoptera
stings are a
common trigger7,15,16
|
|
| OTHER |
Additional symptoms such as cognitive impairment, dizziness,
headache, osteoporosis, musculoskeletal pain, breathing difficulties, anxiety, or depression
may occur7,11,12,17
Please note that this list is not inclusive of all symptoms patients with
ISM may experience
|
Patients with IBS commonly also have anxiety and depression3
|
The information presented here outlines general characteristics of each
disorder. Presentation of signs and symptoms may vary from patient to patient.
Inflammatory Bowel Disease
Inflammatory bowel disease (IBD) is a broad term that includes conditions characterized
by chronic inflammation of the GI tract. IBD
includes Crohn disease and
ulcerative colitis.1
Common Signs and Symptoms
| ISM |
IBD |
| DERMATOLOGIC |

ISM: Maculopapular lesions in an adult2
Monomorphic maculopapular lesions, round, brown or red in color arise
predominantly on the thigh and trunk.
Lesions may spread or spontaneously disappear, which
may or may not indicate disease progression3-5
Symptoms such as flushing, pruritus, and positive Darier sign may be
observed3,5,6
The Darier sign is an important clinical feature of mastocytosis skin
lesions. It is defined by the development of a
wheal-and-flare reaction upon mechanical irritation of the lesion3-5
|
Psoriasis and mucocutaneous lesions associated with IBD can occur7
|
| GASTROINTESTINAL |
GI involvement is commonly reported in patients with ISM5,8,9
Symptoms may include diarrhea, abdominal cramping, bloating,
nausea, and vomiting5,9,10
|
Pain in the lower abdomen, swelling, thickening of the bowel wall,
diarrhea, and rectal bleeding are frequently
reported1,11
|
| SYSTEMIC |
Systemic symptoms include fatigue, anaphylaxis, and weight loss5,9,10,12
Anaphylaxis may occur; patients typically present with hypotensive syncope and without
flushing, urticaria, pruritus, and angioedema5,13,14
Episodes of anaphylaxis appear more likely to develop in patients with mastocytosis
compared to the general population; Hymenoptera stings are a common
trigger5,15,16
|
Weakness, fatigue, and weight changes may be reported1,11
|
| OTHER |
Additional symptoms such as cognitive impairment, dizziness,
headache, osteoporosis, musculoskeletal pain, breathing difficulties,
anxiety, or depression may occur5,10,12,17
Please note that this list is not inclusive of all symptoms patients with
ISM may experience
|
Nutritional deficiencies, anemia, and thromboembolic disease
may occur11,18
|
The information presented here outlines general characteristics of each
disorder. Presentation of signs and symptoms may vary from patient to patient.
Postural Orthostatic Tachycardia Syndrome
Postural orthostatic tachycardia syndrome (POTS) is a chronic multisystem disorder with
orthostatic tachycardia as its cardinal feature.1,2 It
is also
characterized by frequent symptoms of orthostatic intolerance that occur with standing, an increase in
heart rate ≥30 beats per
minute (or ≥40 beats/min for individuals aged 12-19
years old) when moving from recumbent to standing position, and the absence of
orthostatic hypotension (>20/10 mm Hg drop in blood pressure).1,2
Common Signs and Symptoms
| ISM |
POTS |
| DERMATOLOGIC |

ISM: Maculopapular lesions in an adult3
Monomorphic maculopapular lesions, round, brown or red in color arise
predominantly on the thigh and trunk. Lesions may spread or spontaneously disappear, which
may or may not indicate disease progression4-6
Symptoms such as flushing, pruritus, and positive Darier sign may be
observed4.6,7
The Darier sign is an important clinical feature of mastocytosis skin
lesions. It is defined by the development of a
wheal-and-flare reaction upon mechanical irritation of the lesion4-6
|
Some patients may experience episodes of flushing and urticaria1
|
| GASTROINTESTINAL |
GI involvement is commonly reported in patients with ISM6,8,9
Symptoms may include diarrhea, abdominal cramping, bloating,
nausea, and vomiting6,9,10
|
Nausea, bloating, diarrhea, abdominal pain, and vomiting may occur1,2
|
| SYSTEMIC |
Systemic symptoms include fatigue, anaphylaxis, and weight loss6,9-11
Anaphylaxis may occur; patients typically present with hypotensive syncope and without
flushing, urticaria, pruritus, and angioedema6,12,13
Episodes of anaphylaxis appear more likely to develop in patients with mastocytosis
compared to the general population; Hymenoptera stings are a common
trigger6,14,15
|
Symptoms vary between individuals and can include generalized
weakness and fatigue1,2
|
| OTHER |
Additional symptoms such as cognitive impairment, dizziness,
headache, osteoporosis, musculoskeletal pain, breathing difficulties,
anxiety, or depression may occur6,10,11,16
Please note that this list is not inclusive of all symptoms patients with
ISM may experience
|
Some patients with POTS have comorbid conditions or symptoms
associated with abnormal mast cell activation such as dyspnea
and headache1
Other common signs and symptoms are related to orthostatic
intolerance such as light-headedness, palpitations, tremulousness, and
blurred vision1,2
Sleep disturbances, anxiety, tachycardia, tremor, angina-like chest pain,
and migraines may also occur1,2
|
The information presented here outlines general characteristics of each
disorder. Presentation of signs and symptoms may vary from patient to patient.
Idiopathic Anaphylaxis
Idiopathic anaphylaxis (IA) is a multisystem disorder, which presents clinically as
anaphylaxis of unknown etiology. IA is a diagnosis of
exclusion since its
triggers cannot be identified despite a detailed history and careful diagnostic assessment.1,2
Common Signs and Symptoms
| ISM |
IA |
| DERMATOLOGIC |

ISM: Maculopapular lesions in an adult3
Monomorphic maculopapular lesions, round, brown or red in color arise
predominantly on the thigh and trunk. Lesions may spread or spontaneously disappear, which
may or may not indicate disease progression4-6
Symptoms such as flushing, pruritus, and positive Darier sign may be
observed4,6,7
The Darier sign is an important clinical feature of mastocytosis skin
lesions. It is defined by the development of a
wheal-and-flare reaction upon mechanical irritation of the lesion4-6
|
Acute onset of an illness (minutes to several hours) with simultaneous involvement of the
skin, mucosal tissue, or both (eg, generalized hives, pruritus or flushing, swollen
lips-tongue-uvula)1,8
|
| GASTROINTESTINAL |
GI involvement is commonly reported in patients with ISM6,9,10
Symptoms may include diarrhea, abdominal cramping,
bloating,
nausea, and vomiting6,10,11
|
Severe abdominal symptoms such as diarrhea, repetitive vomiting,
nausea, abdominal cramping and pain1,2,8
|
| SYSTEMIC |
Systemic symptoms include fatigue, anaphylaxis, and weight loss6,10-12
Anaphylaxis may occur; patients typically present with hypotensive syncope and without
flushing, urticaria, pruritus, and angioedema6,13,14
Episodes of anaphylaxis appear more likely to develop in patients with mastocytosis
compared to the general population; Hymenoptera stings are a common
trigger6,15,16
|
Systemic symptoms include episodes of anaphylaxis, which may
present as urticaria, angioedema, respiratory compromise,
reduced blood pressure or symptoms of end-organ dysfunction,
and GI manifestations1,8,17
|
| OTHER |
Additional symptoms such as cognitive impairment, dizziness,
headache, osteoporosis, musculoskeletal pain, breathing difficulties, anxiety, or depression
may occur6,11,12,17
Please note that this list is not inclusive of all symptoms patients with
ISM may experience
|
Symptoms of respiratory and/or cardiovascular compromise such as
cough, wheeze, dyspnea and tachycardia, light-headedness, and
shock1,8
Reduced blood pressure and associated symptoms of end-organ
dysfunction may be present as well8
|
Additional Considerations
This section provides some information that may be helpful in further
identifying patients with ISM vs IA and is not inclusive of all distinguishing features. Please refer to
the formal guidelines for each disorder, if available, for a more comprehensive list.
Patients with IA may be diagnosed with SM upon further evaluation. Therefore, patients with recurrent,
unexplained episodes of anaphylaxis should be screened further for the presence of
mastocytosis.18-20